Toe Implants
HemiCAP® Toe, HemiCAP DF and ToeMotion Total Toe Implants











Arthrosurface® offers three different restoration systems to treat toe pain – hallux rigidus: the HemiCAP DF® (Dorsal Flange), the Toe Classic HemiCAP® with no flange and the ToeMotion® Total Toe System. The HemiCAP® Toe Classic is primarily used in early disease where a simple resurfacing will suffice for the lesser metatarsals. The HemiCAP DF® is used in the 1st metatarsal and incorporates an anatomic, extended dorsal curve to improve dorsal roll-off while preventing osteophyte regrowth. For patients with late stage disease who may not want a fusion because of their work or activity demands, Arthrosurface has developed the ToeMotion® Total Toe System. The ToeMotion restores mobility and maintains native biomechanics using the dual curved HemiCAP DF® and modular tray-style phalangeal implant with a threaded baseplate. Fourth generation fixation components provide stable

constructs on both sides of the joint. All Arthrosurface systems are available in a variety of different convexities designed to fit the implant to the patient’s native anatomy. Due to the increasing number of synthetic cartilage revisions, Arthrosurface now offers the BOSS Toe Fixation Post that is used in conjunction with both the HemiCAP DF and ToeMotion Implant Systems. The BOSS Toe Fixation System was specifically designed to fill the distal bone void left behind by synthetic cartilage implants (among others). It is a great solution for patients who want to maintain their motion and avoid a toe fusion.
For the most common type of Foot Arthritis (hallux rigidus), outcome data shows that HemiCAP Toe Implants are the better solution for patients looking to improve motion. The Arthrosurface hemiarthroplasty toe implant systems have a long clinical lifespan, proven fixation and do not burn any bridges for future surgeries such as Toe Fusions.


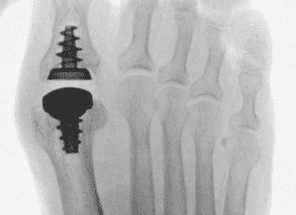
- Screw based implants provide rock solid fixation
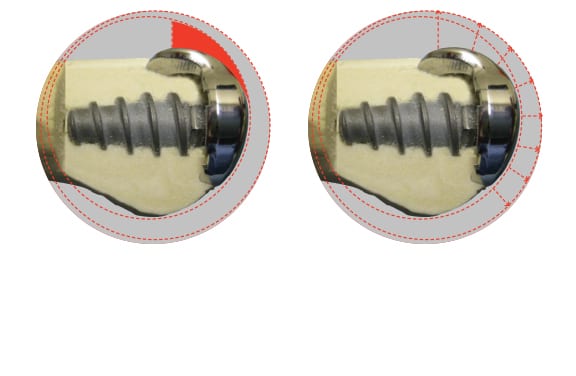
- HemiCAP DF® dual implant curvatures improve dorsal role-off and prevent osteophyte regrowth
- ToeMotion® screw-in baseplate and modular poly inserts provides optimal intraoperative flexibility
- Super smooth articulating cobalt chrome surface to minimize wear on the opposing side
- Conical shaped screw to optimize bone-screw interface
- Inlay arthroplasty and minimal bone removal allows for future fusion if necessary – “No Bridges Burned”
- Anatomic inlay of Toe Classic HemiCAP® maintains the length of the lesser metatarsals
- Standardized thread pitch for precise depth and decompression
- Proven clinical history with over 20,000 MTP implants
HemiCAP® technology was designed so patients can continue working and retain an active lifestyle without compromising future treatments.
- May be performed on an outpatient basis
- Data shows the HemiCAP Toe Implant as the better solution for patients looking to improve motion when compared to Cartiva SCI
- Allows for preservation of bone and soft tissues
- Bridges the gap between biological therapies and joint fusion
- Clinical studies demonstrate positive clinical outcomes at 5-7 years
- Maintains existing joint biomechanics thereby allowing normal motion
- Patients experience a rapid return to activity for both work and exercise
- Patients report pain relief, rapid recovery and range of motion improvements
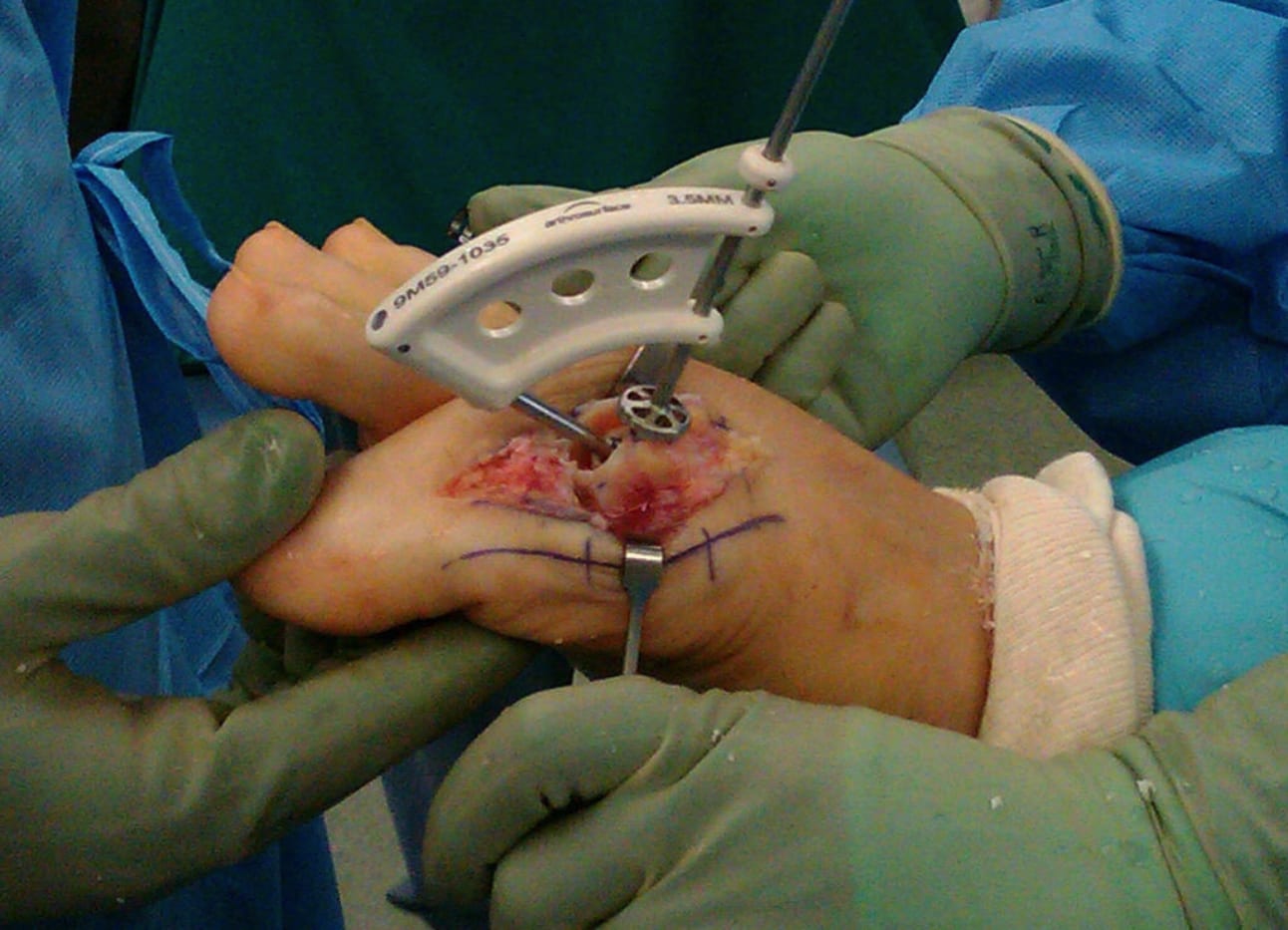
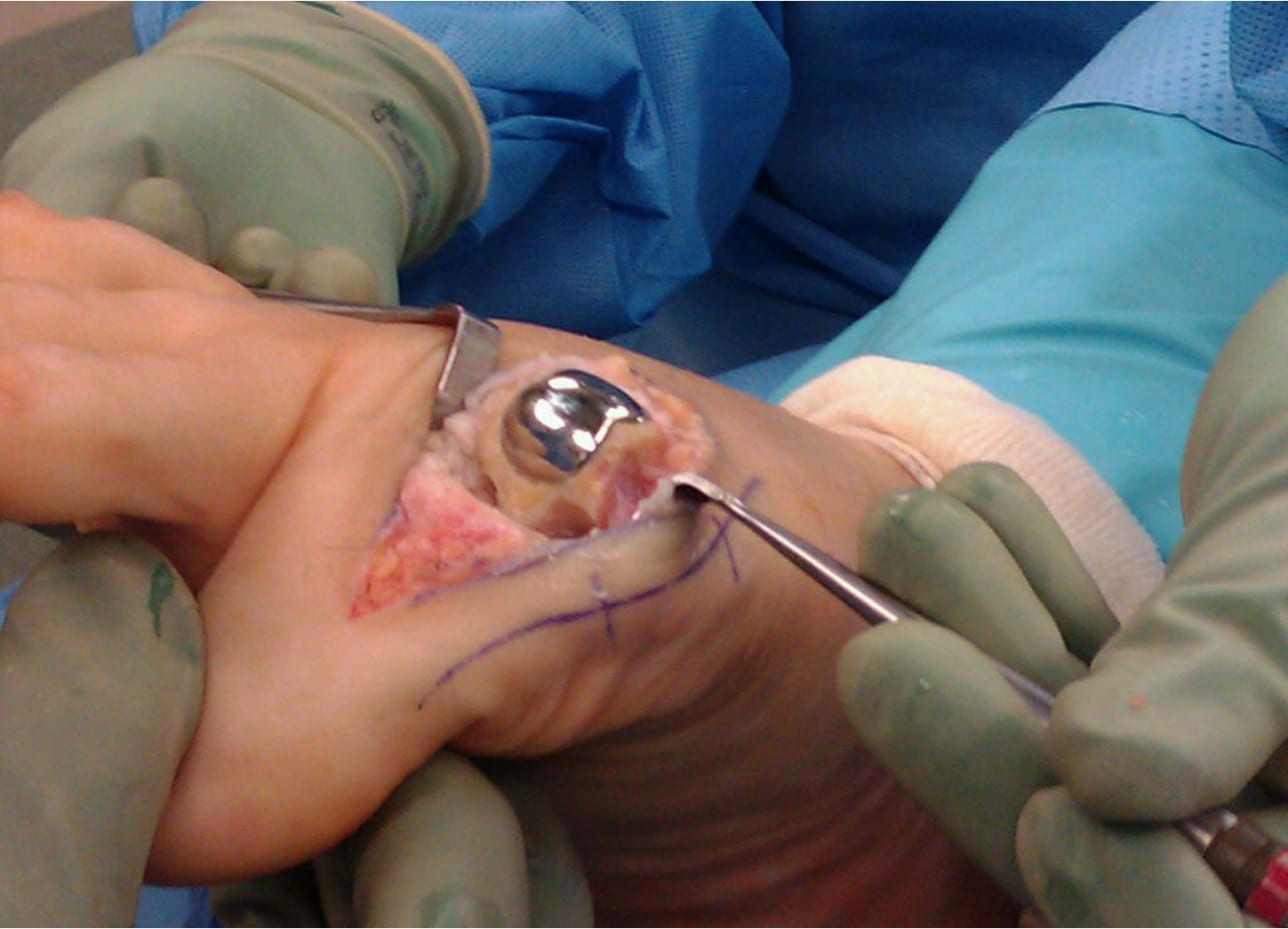
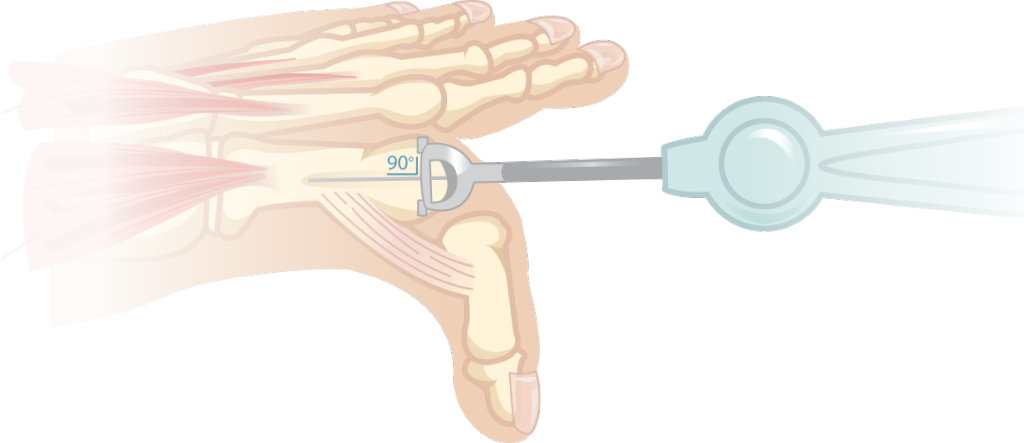 The Toe HemiCAP® implant system is comprised of two parts, an articular cap and a fixation component. The instruments are organized in the order of surgery, proceeding from left to right and top to bottom. The procedure begins with a guide to identify the size of the metatarsal head. Then place the guide wire perpendicular to the head. A step drill is used to prepare the screw hole before the fixation component is advanced (joint decompression can be adjusted by advancing the screw 2-4mm). The uniquely designed instruments are used to map the contours of the patient’s native surface curvatures using the fixation component as a central axis. A reamer then removes the damaged cartilage to create a socket for the implant. If using the DF HemiCAP®, a second reamer is inserted into the screw to ream the dorsal socket. Place the trial to assess proper implant fit. After, any osteophytes or boney edges are trimmed off around the implant so bone and cartilage surfaces surrounding the implant are flush. (If you are using the ToeMotion Total Toe System, skip impacting the DF implant and contiune on to the next paragraph). If you are only implanting the DF HemiCAP®, once the surface preparation is complete, the implant is positioned and seated with several taps of the mallet. The ToeMotion™ phalangeal component is prepared in a similar manner. A guidewire is placed perpendicular to the phalangeal surface. A reamer is then used to prepare a socket until the reamer is slightly recessed to the surrounding surface. The sutures of the sterile delivery tool are then placed behind the phalangeal component and this metal baseplate is then screwed into place so that the final implant is slightly recessed. Plastic trials are then placed into the baseplate and a range of motion is performed to assess which insert is best for the patient. Once the proper insert is chosen it is placed into baseplate, the delivery tool is then cinched down against the implant and the lead sutures are then twisted until an audible click is heard which means the poly has locked into the baseplate. The DF HemiCAP® is then impacted onto the metatarsal taper post to lock the morse taper. The wound is then closed.
The Toe HemiCAP® implant system is comprised of two parts, an articular cap and a fixation component. The instruments are organized in the order of surgery, proceeding from left to right and top to bottom. The procedure begins with a guide to identify the size of the metatarsal head. Then place the guide wire perpendicular to the head. A step drill is used to prepare the screw hole before the fixation component is advanced (joint decompression can be adjusted by advancing the screw 2-4mm). The uniquely designed instruments are used to map the contours of the patient’s native surface curvatures using the fixation component as a central axis. A reamer then removes the damaged cartilage to create a socket for the implant. If using the DF HemiCAP®, a second reamer is inserted into the screw to ream the dorsal socket. Place the trial to assess proper implant fit. After, any osteophytes or boney edges are trimmed off around the implant so bone and cartilage surfaces surrounding the implant are flush. (If you are using the ToeMotion Total Toe System, skip impacting the DF implant and contiune on to the next paragraph). If you are only implanting the DF HemiCAP®, once the surface preparation is complete, the implant is positioned and seated with several taps of the mallet. The ToeMotion™ phalangeal component is prepared in a similar manner. A guidewire is placed perpendicular to the phalangeal surface. A reamer is then used to prepare a socket until the reamer is slightly recessed to the surrounding surface. The sutures of the sterile delivery tool are then placed behind the phalangeal component and this metal baseplate is then screwed into place so that the final implant is slightly recessed. Plastic trials are then placed into the baseplate and a range of motion is performed to assess which insert is best for the patient. Once the proper insert is chosen it is placed into baseplate, the delivery tool is then cinched down against the implant and the lead sutures are then twisted until an audible click is heard which means the poly has locked into the baseplate. The DF HemiCAP® is then impacted onto the metatarsal taper post to lock the morse taper. The wound is then closed.
Click here to download the Toe HemiCAP DF & ToeMotion Surgical Technique Guide
Click here to download the Toe Classic Surgical Technique Guide
- The HemiCAP® procedure is intuitive and easy to learn
- The minimally invasive outpatient procedure typically takes less than an hour
- Soft-tissue envelope and native joint biomechanics are maintained
- Skeletal anatomy and bone stock are preserved allowing future fusion or total toe
- Phalangeal surface reamer allows for a controlled cheilectomy
- The two components are connected together via morse taper, with zero reported loosening